
Page 43 - Real_Reading_1
P. 43
Umfitf O I'd lilre to resister
B The medical questionnaire
1 You are going to complete a medical questionnaire. This includes the following
words. Make sure you know what they mean. Use a dictionary if necessary.
operation pregnancy disability prescription allergy medication heart attack stroke
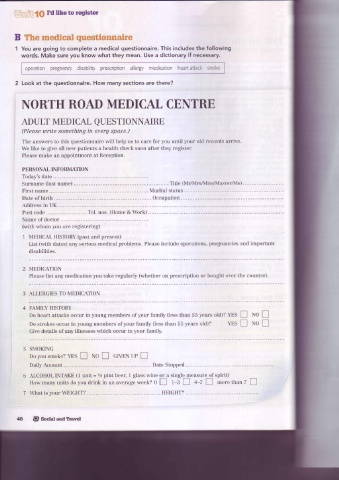
Look at the questionnaire. How many sections are there?
i NORTH ROAD MEDICAL CENTRE
ADULT MEDICAL
QUESTIONNAIRE
(Please write something in euery space.)
The answers to this questionnaire will help us to care for you until your old records arrive.
We like to give all new patients a health check soon after they register.
Please make an appointment at Reception.
PERSONAL INFORMATION
.
d
Today's ate ..........
Surname 0ast name) .. Title (Mr/NIrs/IvIisVMaster/N'Is)
First name . . . . Marital status .. ... . .. .
Date of birth ... Occupation...............
i
Addressn UK.........
Post code ...... Tel. nos. (Home & Work)
Narne of doctor
(with whom you are registering)
1 MEDICAL HISTORY (past and present)
List (with dates) any serious medical problems. Please include operations, pregnancies and important
disabilities.
2 MEDICATION
Please list any medication you take regularly (whether on prescription or bought over the counter).
3 ALLERGIES TO MEDICATION
FAMILY HISTORY
Do heart attacks occur in young members of your family (less than 55 years old)? YES I rvol
Do strokes occur in young members of your family (less than 55 years old)? YES I NoI
Give details of any illnesses which occur in your family.
SMOKING
Do you smoke? YES E No I GIVEN uP I
Daily Amount Date Stopped
ALCOHOL INTAKE (1 unit = 1/z pinl beer, 1 glass wine or a single measure of spirit)
How many units do you drink in an average week? 0 [ 1-3 I 4-7 J more than 7 [
7 \{hat is your WEIGHT? ....... HEIGHT?
@ Sociat andTravel